Enhancing horse safety in training and racing
The Gerald Leigh Memorial Lectures 2023

Article by Adam Jackson MRCVS
The Gerald Leigh Memorial Lectures, is an annual gathering devoted to the racing industry and the health and wellbeing of the horses involved.
This year, equine veterinarians, researchers, students and industry professionals from around the world attended the event, held June 8, 2023, at the historic Tattersalls Sales in Newmarket, England.

There were insightful and informative lectures that educated the attendants but also instigated a healthy, lively debate on the health and welfare of the training and competing of horses. The underlying theme that was present during the whole event was all members of the conference had a deep passion and commitment to continuously progress and improve on managing the welfare and wellbeing of the horses in the industry, both on and off of the track.
Two very special guest speakers, Sir Mark Prescott and Luca Cumani, wonderfully illustrated these sentiments as they described their reflections on the improvement and enhancement of horse safety.
Horse racing may be regarded as an elite sport, and all activities involving horses have an element of risk. All stakeholders in the racing industry must continuously work to ensure that the risks are minimized in order to reduce the number of injuries and fatalities that may occur in training and on the racecourse. There are now well-publicized concerns regarding the acceptability of exposing horses to risk in racing. These lectures and all of the attendees embraced the values of the public will so that there can be continued acceptance of horse sports.
Reducing the Incidence of Fractures in Racing
Christopher Riggs of The Hong Kong Jockey Club clearly outlined the various strategies to reduce the risk of fractures in racehorses. There are two principal strategies that may used to reduce the incidence of severe fractures in horses while racing and training:
1.Identifying extrinsic factors that increase risk and take action to minimize them.
An example would be investigating different racing surfaces in order to determine which may provide the safest racing surface. However, studies have provided limited evidence and support for subtle extrinsic factors.
2.Identifying individuals that are at increased risk and prevent them from racing or minimize that risk until the risk has subsided.

There are many research routes that are being undertaken to identify those horses that may be at a higher risk of fractures. There are investigations involving heritability and molecular studies that may provide evidence of genetic predisposition to fracture. However, Dr. Riggs explained that further understanding of the relationship between genetic, epigenetic and environmental factors is required before genetic screening is likely to be of practical use.
Pre-race screening of horses by diligent clinical examination is poor at reducing the incidence of fracture. Dr. Riggs described another strategy that may assist with a clinical examination that is the use of biomarkers in blood and urine.
Unfortunately, the precision to be of practical value has so far remained relatively unrewarding. Wearable technology that records biometric parameters, including stride characteristics, has shown some promise in identifying horses that are at increased risk of fracture; although Dr. Riggs explained that this work requires further development.
Finally, Dr. Riggs described both the use and current limitations of diagnostic imaging in identifying pre-fracture pathology in order to identify a horse at imminent risk of fracture. He conceded that further knowledge of the significance of the range of abnormalities that can be detected by imaging is incomplete.
Dr. Riggs concluded his lecture by expressing that the implementation of diagnostic imaging to screen “high-risk” horses identified through genetic, epidemiology, biomarkers and/or biometrics may be the best hope to reduce the incidence of racing fractures. This field can be advanced with further studies, especially of a longitudinal nature.
Professor Tim Barker of Bristol Veterinary School discussed the need for further investment in welfare research and education. One avenue of investment that should be seriously considered is the analysis of data related to (fatal) injuries in Thoroughbred racing over the last 25 years.
It was expressed, with the abundance of data that has been collected, that some risk factors would be relatively simple to identify. An encouraging example in the collection and use of data to develop models in predicting and potentially preventing injury has been conducted by the Hong Kong Jockey Club funded by the Hong Kong Jockey Club Equine Welfare Research Foundation. This may provide an opportunity to pilot the use of risk profiling to contribute to decision-making about race entries. In addition, the results of the pilot study combined with other sources of data may encourage race authorities to mandate the collection of veterinary and training data in order to help in risk mitigation.
Horse racing is an international sport, and there are different governing bodies that ensure racing integrity. However, the concept of social license equestrian sports and Thoroughbred horse racing continues to gain significant public attention. Therefore, racing governing bodies are increasingly aiming to provide societal assurances on equine welfare.
Dr. Ramzan of Rossdales Veterinary Surgeons provided an eloquent and clear message during his lecture that race yard veterinarians and trainers are instrumental in ensuring good horse health and welfare and reducing serious injury of the horse both while training or racing, which will provide sufficient trust and legitimacy from the public and society. This feasible goal can be reached with good awareness of members involved in the care and training of each individual horse and conveying this information and any concerns to their veterinarian. The veterinarian can also contribute by honing their knowledge and skills and working closely with yard staff in order to make appropriate and better targeted veterinary intervention.
In the last two decades, there has been an incredible evolution and exciting developments in diagnostic imaging in the veterinary profession. It is believed that these technologies can provide a significant contribution to helping in mitigating fracture risks to racehorses on the course and in training.
Professor Mathieu Spriet of University of California, Davis, described how these improvements in diagnostic imaging has led to the detection of early lesions as well as allowing the monitoring of the lesions’ evolution.

He continued by explaining the strengths and limitations of different imaging modalities such as computed tomography (CT), magnetic resonance imaging (MRI) and positron emission tomography (PET). Being one of the leaders in the use of PET in equine veterinary medicine, he presented further insight on how this particular modality provides high-resolution 3-D bone scans while being very sensitive to the identification of bone turn-over prior to the development of structural changes and allowing one to distinguish between active and inactive processes when structural changes are present.
He concluded his impressive lecture by providing evidence with amazing PET images that the role of imaging is not merely for diagnostic purposes to characterize clinical abnormalities, but can also be used as a screening tool in certain horse populations for fracture risk assessment or for the monitoring of lesions to provide clearance for racing.
Fractures, due to bone overloading rather than direct trauma occur commonly in Thoroughbred racehorses and are the leading cause of euthanasia on the racecourse. Despite many changes to race conditions, the number of catastrophic fractures has remained relatively static, with approximately 60 horses a year having a fatal fracture during a race in the UK.
Against this backdrop, there have been great developments in the diagnosis and treatment of fractures in the last 40 years. Prevention of racecourse and training fractures would be ideal so the development of efficacious techniques to screen horses at risk may reduce the incidence and preserve social licensing.

Dr. Ian Wright
One technique discussed by Dr. Ian Wright of Newmarket Equine Referrals was to help mitigate the impact of racecourse fractures, which would be acute immobilization of racecourse fractures, thus, reducing associated pain and anxiety while optimizing clinical outcome and reducing on course fatality rates. Because of our increased understanding of fracture pathogenesis and their associated biomechanics, effective fracture immobilization has been made possible. The majority of fractures that occur in flat racing and between obstacles in jump racing, are a result of stress or fatigue failure of the bone and not associated with trauma.
In addition, fractures seen on the racecourse are often found in the same specific sites (i.e., metacarpal/metatarsal condyles and the proximal sesamoid bones of the fetlock) and have repeatable configurations. With this understanding and knowledge, racecourse veterinarians can optimally immobilize a fracture in a logical and pre-planned manner.
As Dr. Wright expressed, this allows the fracture patient to have reduced pain and anxiety and enable the horse to be moved from the course comfortably so that it can be further examined. Ultimately, this allows the veterinarian and all stakeholders to make effective and judicious decisions for the sake of the horse’s welfare and wellbeing. As Dr. Wright concluded, this benefits both horses and racing.
Dr. Debbie Guest of the Royal Veterinary College discussed a different approach in mitigating the risk of fractures during training and racing by developing novel tools to reduce catastrophic fractures Thoroughbreds. Because it has been found that some horses are more inherently predisposed to fractures than other horses, Dr. Guest and her team have developed a genome-wide polygenic risk score so that one can potentially calculate an individual horse’s risk of fracturing during training or racing compared to the population as a whole.
This strategy may contribute in identifying genetically high-risk horses so that additional monitoring of the patients can be exercised during their careers and also leading to fracture risk, which are found to be the cause of approximately half of these incidents.
The system of using DNA testing to identify biological processes that may or may not be present ultimately leading to fracture risk may be a powerful tool in lowering the risk of catastrophic fracture and requires further research and application.
Cardiac events & sudden cardiac death in training and racing

In racehorses, sudden death that is associated with exercise on the racetrack or during training is a serious risk to jockeys and adversely affects horse welfare and the public perception of the sport. It is believed 75% of race day fatalities result from euthanasia following a catastrophic injury. The other 25% of fatalities is due to sudden deaths and cardiac arrhythmias are found to be the cause of approximately half of these incidents. The lectures focused on this area of concern by providing three interesting lectures on cardiac issues in the racehorse industry.
Dr. Laura Nath of the University of Adelaide, explained the difficulties in identifying horses that are at risk of sudden cardiac death. It is believed that part of the solution to this difficult issue is the further development and use of wearable devices including ECG and heart rate monitors.
With the use of these technologies, the goal would be to recognize those horses that are not progressing appropriately through their training and screen these horses for further evaluation. This course of action has been seen in human athletes that develop irregular rhythms that are known to cause sudden cardiac death with the use of computational ECG analysis, even when the ECGs appear normal on initial visual inspection.
Knowing that ECGs and particularly P-waves are used as a non-invasive electrocardiographic marker for atrial remodeling in humans, Dr. Nath recently completed a study on the analysis variations in the P-wave seen on ECGs in athletic horses and found that increases of P-waves in racehorses are associated with structural and electrical remodeling in the heart and may increase the risk of atrial fibrillation (cardiac event).
Dr. Celia Marr of Rossdales Veterinary Surgeons continued the discussion of cardiac disease in both the training and racing of horses. Unfortunately, cardiac disease knowledge does lag compared to musculoskeletal and respiratory diseases when considering the causes of poor performance in racehorses. Due to the fact that cardiac rhythm disturbances are fairly common, occurring in around 5–10% of training sessions in healthy horses in Newmarket and over 50% of horses investigated for poor performance, Dr. Marr expressed the need for further research and investigation in this area.
In addition, this research needs to determine if there is indeed a link between heart rhythm disturbances and repeated episodes of poor performance and sudden cardiac arrest. ECGs and associated technologies are helpful, but there are limitations such as the fact that rhythm disturbances do not always occur every time the horse is exercised. Therefore, it would be of great value that a robust criterion is established when evaluating ECGs in racehorses. The Horserace Betting Levy Board has provided funding for investigation by initially exploring the natural history of paroxysmal atrial fibrillation (self-correcting form) to understand risk factors and predict outcomes for affected horses.
Continuing the theme of the lectures on irregular heart rhythms and associated sudden cardiac death (SCD) in training and racing, Professor Kamalan Jeevaratnam described his exciting research in using artificial intelligence (AI) to identify horses at increased risk of developing irregular rhythms that may cause SCD.

AI is an exciting and rapidly expanding field of computer science that is beginning to be implemented in veterinary medicine. With funding by the Horserace Betting Levy Board and the Grayson Jockey Club Research Foundation, Professor Jeevaratnam of the University of Surrey, has piloted three novel algorithms that help predict horses with rhythm abnormalities through the analysis of horses’ ECGs.
It was acknowledged that further research is required to develop this technology by using data collected from multiple sources, but the initial results are promising in the development of an useful AI tool to identify horses at risk of SCD and prevent catastrophic events, thus, ensuring the welfare of the horse in racing.
Conclusion
The Gerald Leigh Memorial Lectures was a thoroughly successful and enjoyable event attended by a variety of different members of the horse racing industry. Not only did the lecturers provide interesting and valuable information but also excitement for the future of racing. It was very clear that all the lecturers and attendees were passionate and committed to the racehorse welfare and wellbeing as well as retaining the social license for an exciting sport.
EIPH - could there be links to sudden death and pulmonary haemorrhage?
Dr Peter W. Physick-Sheard, BVSc, FRCVS, explores preliminary research and hypotheses, being conducted by the University of Guelph, to see if there is a possibility that these conditions are linked and what this could mean for future management and training of thoroughbreds.

"World's Your Oyster,” a three-year-old thoroughbred mare, presented at the veterinary hospital for clinical examination. She won her maiden start as a two-year-old and placed once in two subsequent starts. After training well as a three-year-old, she failed to finish her first start, easing at the top of the stretch, and was observed to fade abruptly during training. Some irregularity was suspected in heart rhythm after exercise. Thorough clinical examination, blood work, ultrasound of the heart and an ECG during rest and workout revealed nothing unusual.
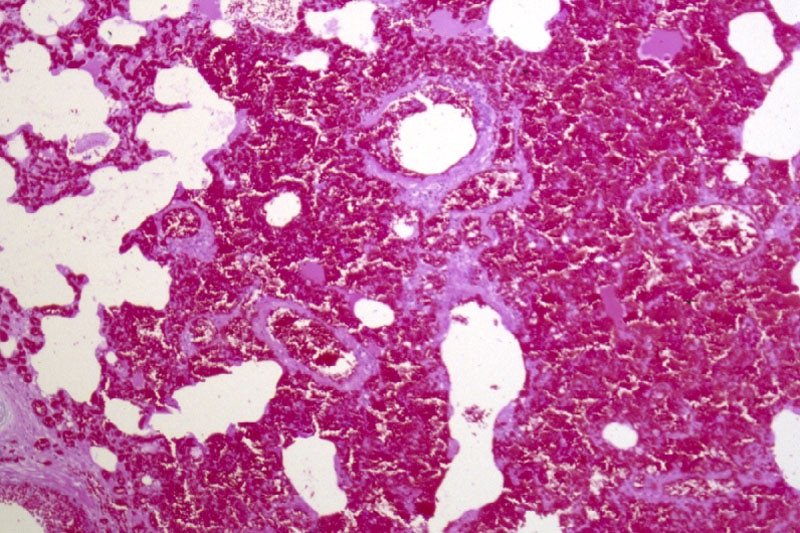
Returning to training, Oyster placed in six of her subsequent eight starts, winning the last two. She subsequently died suddenly during early training as a four-year-old. At post-mortem, diagnoses of pulmonary haemorrhage and exercise-induced pulmonary haemorrhage were established—a very frustrating and unfortunate outcome.

Across the racing world, a case like this probably occurs daily. Anything that can limit a horse's ability to express its genetic potential is a major source of anxiety when training. The possibility of injury and lameness is the greatest concern, but a close second is respiratory disease, with bleeding from the lungs (most often referred to as exercise induced pulmonary [lung] haemorrhage or EIPH) being high on the list.
EIPH is thought to occur in as many as 85 percent of racehorses, and may initially be very mild without obvious clinical consequences. In some cases it can be associated with haemorrhage of sufficient severity for blood to appear at the nostrils, even at first occurrence. In many racing jurisdictions this is a potentially career-ending problem. In these horses, an impact on performance is unquestionable. Bleeding from the lungs is the reason for the existence of ‘Lasix programs,’ involving pre-race administration of a medication considered to reduce haemorrhage. Such programs are controversial—the justifications for their existence ranging from addressing welfare concerns for the horse to dealing with the performance impacts.
Much less frequently encountered is heavy exercise-associated bleeding from the nostrils (referred to as epistaxis), which can sometimes be accompanied by sudden death, during or shortly after exercise. Some horses bleed heavily internally and die without blood appearing at the nostrils. Haemorrhage may only become obvious when the horse is lying on its side, or not until post-mortem. Affected animals do not necessarily have any history of EIPH, either clinically or sub-clinically. There is an additional group of rare cases in which a horse simply dies suddenly, most often very soon after work and even after a winning performance, and in which little to nothing clearly explains the cause on post-mortem. This is despite the fact most racing jurisdictions study sudden death cases very closely.
EIPH is diagnosed most often by bronchoscopy—passing an endoscope into the lung after work and taking a look. In suspected but mild cases, there may not be sufficient haemorrhage to be visible, and a procedure called a bronchoalveolar lavage is performed. The airways are rinsed and fluid is collected and examined microscopically to identify signs of bleeding. Scoping to confirm diagnosis is usually a minimum requirement before a horse can be placed on a Lasix program.
Are EIPH, severe pulmonary haemorrhage and sudden death related? Are they the same or different conditions?
At the University of Guelph, we are working on the hypothesis that most often they are not different—that it’s degrees of the same condition, or closely related conditions perhaps with a common underlying cause. We see varying clinical signs as being essentially a reflection of severity and speed of onset of underlying problems.

Causes in individual cases may reflect multiple factors, so coming at the issues from several different directions, as is the case with the range of ongoing studies, is a good way to go so long as study subjects and cases are comparable and thoroughly documented. However, starting from the hypothesis that these may all represent basically the same clinical condition, we are approaching the problem from a clinical perspective, which is that cardiac dysfunction is the common cause.
Numerous cardiac disorders and cellular mechanisms have the potential to contribute to transient or complete pump (heart) failure. However, identifying them as potential disease candidates does not specifically identify the role they may have played, if any, in a case of heart failure and in lung haemorrhage; it only means that they are potential primary underlying triggers. It isn't possible for us to be right there when a haemorrhage event occurs, so almost invariably we are left looking at the outcome—the event of interest has passed. These concerns influence the approach we are taking.
Background
The superlative performance ability of a horse depends on many physical factors:
Huge ventilatory (ability to move air) and gas exchange capacity
Body structure including limb length and design - allows it to cover ground rapidly with a long stride
Metabolic adaptations - supports a high rate of energy production by burning oxygen, tolerance of severe metabolic disruptions toward the end of race-intensity effort
High cardiovascular capacity - allows the average horse to pump roughly a brimming bathtub of blood every minute
At race intensity effort, these mechanisms, and more, have to work in coordination to support performance. There is likely not much reserve left—two furlongs (400m) from the winning post—even in the best of horses. There are many wild cards, from how the horse is feeling on race day to how the race plays out; and in all horses there will be a ceiling to performance. That ceiling—the factor limiting performance—may differ from horse to horse and even from day to day. There’s no guarantee that in any particular competition circumstances will allow the horse to perform within its own limitations. One of these factors involves the left side of the heart, from which blood is driven around the body to the muscles.
A weak link - filling the left ventricle
The cardiovascular system of the horse exhibits features that help sustain a high cardiac output at peak effort. The feature of concern here is the high exercise pressure in the circulation from the right ventricle, through the lungs to the left ventricle. At intense effort and high heart rates, there is very little time available to fill the left ventricle—sometimes as little as 1/10 of a second; and if the chamber cannot fill properly, it cannot empty properly and cardiac output will fall. The circumstances required to achieve adequate filling include the readiness of the chamber to relax to accept blood—its ‘stiffness.’ Chamber stiffness increases greatly at exercise, and this stiffened chamber must relax rapidly in order to fill. That relaxation seems not to be sufficient on its own in the horse at high heart rates. Increased filling pressure from the circulation draining the lungs is also required. But there is a weak point: the pulmonary capillaries.

These are tiny vessels conducting blood across the lungs from the pulmonary artery to the pulmonary veins. During this transit, all the gas exchange needed to support exercise takes place. The physiology of other species tells us that the trained lung circulation achieves maximum flow (equivalent to cardiac output) by reducing resistance in those small vessels. This process effectively increases lung blood flow reserve by, among other things, dilating small vessels. Effectively, resistance to the flow of blood through the lungs is minimised. We know this occurs in horses as it does in other species; yet in the horse, blood pressure in the lungs still increases dramatically at exercise.
If this increase is not the result of resistance in the small vessels, it must reflect something else, and that appears to be resistance to flow into the left chamber. This means the entire lung circulation is exposed to the same pressures, including the thin-walled capillaries. Capillaries normally work at quite low pressure, but in the exercising horse, they must tolerate very high pressures. They have thin walls and little between them, and the air exchange sacs in the lung. This makes them vulnerable. It's not surprising they sometimes rupture, resulting in lung haemorrhage.

Recent studies identified changes in the structure of small veins through which the blood flows from the capillaries and on toward the left chamber. This was suspected to be a pathology and part of the long-term consequences of EIPH, or perhaps even part of the cause as the changes were first identified in EIPH cases. It could be, however, that remodelling is a normal response to the very high blood flow through the lungs—a way of increasing lung flow reserve, which is an important determinant of maximum rate of aerobic working.
The more lung flow reserve, the more cardiac output and the more aerobic work an animal can perform. The same vein changes have been observed in non-racing horses and horses without any history or signs of bleeding. They may even be an indication that everything is proceeding as required and a predictable consequence of intense aerobic training. On the other hand, they may be an indication in some horses that the rate of exercise blood flow through their lungs is a little more than they can tolerate, necessitating some restructuring. We have lots to learn on this point.
If the capacity to accommodate blood flow through the lungs is critical, and limiting, then anything that further compromises this process is likely to be of major importance. It starts to sound very much as though the horse has a design problem, but we shouldn't rush to judgement. Horses were probably not designed for the very intense and sustained effort we ask of them in a race. Real-world situations that would have driven their evolution would have required a sprint performance (to avoid ambush predators such as lions) or a prolonged slower-paced performance to evade predators such as wolves, with only the unlucky victim being pushed to the limit and not the entire herd.
Lung blood flow and pulmonary oedema
There is another important element to this story. High pressures in the capillaries in the lung will be associated with significant movement of fluid from the capillaries into lung tissue spaces. This movement in fact happens continuously at all levels of effort and throughout the body—it's a normal process. It's the reason the skin on your ankles ‘sticks’ to the underlying structures when you are standing for a long time. So long as you keep moving a little, the lymphatic system will draw away the fluid.
In a diseased lung, tissue fluid accumulation is referred to as pulmonary oedema, and its presence or absence has often been used to help characterise lung pathologies. The lung lymphatic system can be overwhelmed when tissue fluid is produced very rapidly. When a horse experiences sudden heart failure, such as when the supporting structures of a critical valve fail, one result is massive overproduction of lung tissue fluid and appearance of copious amounts of bloody fluid from the nostrils.
The increase in capillary pressure under these conditions is as great as at exercise, but the horse is at rest. So why is there no bloody fluid in the average, normal horse after a race? It’s because this system operates very efficiently at the high respiratory rates found during work: tissue fluid is pumped back into the circulation, and fluid does not accumulate. The fluid is pumped out as quickly as it is formed. An animal’s level of physical activity at the time problems develop can therefore make a profound difference to the clinical signs seen and to the pathology.
Usual events with unusual consequences
If filling the left ventricle and the ability of the lungs to accommodate high flow at exercise are limiting factors, surely this affects all horses. So why do we see such a wide range of clinical pictures, from normal to subclinical haemorrhage to sudden death?
Variation in contributing factors such as type of horse, type and intensity of work, sudden and unanticipated changes in work intensity, level of training in relation to work and the presence of disease states are all variables that could influence when and how clinical signs are seen, but there are other considerations.
Although we talk about heart rate as a fairly stable event, there is in fact quite a lot of variation from beat to beat. This is often referred to as heart rate variability. There has been a lot of work performed on the magnitude of this variability at rest and in response to various short-term disturbances and at light exercise in the horse, but not a lot at maximal exercise. Sustained heart rate can be very high in a strenuously working horse, with beats seeming to follow each other in a very consistent manner, but there is in fact still variation.
Some of this variation is normal and reflects the influence of factors such as respiration. However, other variations in rate can reflect changes in heart rhythm. Still other variations may not seem to change rhythm at all but may instead reflect the way electrical signals are being conducted through the heart.
These may be evident from the ECG but would not appear abnormal on a heart rate monitor or when listening. These variations, whether physiologic (normal) or a reflection of abnormal function, will have a presently, poorly understood influence on blood flow through the lungs and heart—and on cardiac filling. Influences may be minimal at low rates, but what happens at a heart rate over 200 and in an animal working at the limits of its capacity?
Normal electrical activation of the heart follows a pattern that results in an orderly sequence of heart muscle contraction, and that provides optimal emptying of the ventricles. Chamber relaxation complements this process.
An abnormal beat or abnormal interval can compromise filling and/or emptying of the left ventricle, leaving more blood to be discharged in the next cycle and back up through the lungs, raising pulmonary venous pressure. A sequence of abnormal beats can lead to a progressive backup of blood, and there may not be the capacity to hold it—even for one quarter of a second, a whole cardiac cycle at 240 beats per minute.
For a horse that has a history of bleeding and happens to be already functioning at a very marginal level, even minor disturbances in heart rhythm might therefore have an impact. Horses with airway disease or upper airway obstructions, such as roarers, might find themselves in a similar position. An animal that has not bled previously might bleed a little, one that has a history of bleeding may start again, or a chronic bleeder may worsen.
Relatively minor disturbances in cardiac function, therefore, might contribute to or even cause EIPH. If a horse is in relatively tough company or runs a hard race, this may also contribute to the onset or worsening of problems. Simply put, it's never a level playing field if you are running on the edge.
Severe bleeding
It has been suspected for many years that cases of horses dying suddenly at exercise represent sudden-onset cardiac dysfunction—most likely a rhythm disturbance. If the rhythm is disturbed, the closely linked and carefully orchestrated sequence of events that leads to filling of the left ventricle is also disturbed. A disturbance in cardiac electrical conduction would have a similar effect, such as one causing the two sides of the heart to fall out of step, even though the rhythm of the heart may seem normal.
The cases of horses that bleed profusely at exercise and even those that die suddenly without any post-mortem findings can be seen to follow naturally from this chain of events. If the changes in heart rhythm or conduction are sufficient, in some cases to cause massive pulmonary haemorrhage, they may be sufficient in other cases to cause collapse and death even before the horse has time to exhibit epistaxis or even clear evidence of bleeding into the lungs.

EIPH and dying suddenly
If these events are (sometimes) related, why is it that some horses that die of pulmonary haemorrhage with epistaxis do not show evidence of chronic EIPH? This is one of those $40,000 questions. It could be that young horses have had limited opportunity to develop chronic EIPH; it may be that we are wrong and the conditions are entirely unrelated. But it seems more likely that in these cases, the rhythm or conduction disturbance was sufficiently severe and/or rapid in onset to cause a precipitous fall in blood pressure with the animal passing out and dying rapidly.
In this interpretation of events, the missing link is the heart. There is no finite cutoff at which a case ceases to be EIPH and becomes pulmonary haemorrhage. Similarly, there is no distinct point at which any case ceases to be severe EIPH and becomes EAFPH (exercise-associated fatal pulmonary haemorrhage). In truth, there may simply be gradation obscured somewhat by variable definitions and examination protocols and interpretations.
The timing of death
It seems from the above that death should most likely take place during work, and it often does, but not always. It may occur at rest, after exercise. Death ought to occur more often in racing, but it doesn't.
The intensity of effort is only one factor in this hypothesis of acute cardiac or pump failure. We also have to consider factors such as when rhythm disturbances are most likely to occur (during recovery is a favourite time) and death during training is more often a problem than during a race.
A somewhat hidden ingredient in this equation is possibly the animal's level of emotional arousal, which is known to be a risk factor in humans for similar disturbances. There is evidence that emotions/psychological factors might be much more important in horses than previously considered. Going out for a workout might be more stimulating for a racehorse than a race because before a race, there is much more buildup and the horse has more time to adequately warm up psychologically. And then, of course, temperament also needs to be considered. These are yet further reasons that we have a great deal to learn.

Our strategy at the University of Guelph
These problems are something we cannot afford to tolerate, for numerous reasons—from perspectives of welfare and public perception to rider safety and economics. Our aim is to increase our understanding of cardiac contributions by identifying sensitive markers that will enable us to say with confidence whether cardiac dysfunction—basically transient or complete heart failure—has played a role in acute events.
We are also looking for evidence of compromised cardiac function in all horses, from those that appear normal and perform well, through those that experience haemorrhage, to those that die suddenly without apparent cause. Our hope is that we can not only identify horses at risk, but also focus further work on the role of the heart as well as the significance of specific mechanisms. And we hope to better understand possible cardiac contributions to EIPH in the process. This will involve digging deeply into some aspects of cellular function in the heart muscle, the myocardium of the horse, as well as studying ECG features that may provide insight and direction.
Fundraising is underway to generate seed money for matching fund proposals, and grant applications are in preparation for specific, targeted investigations. Our studies complement those being carried out in numerous, different centres around the world and hopefully will fill in further pieces of the puzzle. This is, indeed, a huge jigsaw, but we are proceeding on the basis that you can eat an elephant if you're prepared to process one bite at a time.
How can you help? Funding is an eternal issue. For all the money that is invested in horses there is a surprisingly limited contribution made to research and development—something that is a mainstay of virtually every other industry; and this is an industry.
Look carefully at the opportunities for you to make a contribution to research in your area. Consider supporting studies by making your experience, expertise and horses available for data collection and minimally invasive procedures such as blood sampling.
Connect with the researchers in your area and find out how you can help. Watch your horses closely and contemplate what they might be telling you—it's easy to start believing in ourselves and to stop asking questions. Keep meticulous records of events involving horses in your care— you never know when you may come across something highly significant. And work with researchers (which often includes track practitioners) to make your data available for study.
Remember that veterinarians and university faculty are bound by rules of confidentiality, which means what you tell them should never be ascribed to you or your horses and will only be used without any attribution, anonymously. And when researchers reach out to you to tell you what they have found and to get your reactions, consider actually attending the sessions and participating in the discussion; we can all benefit—especially the ultimate beneficiary which should be the horse. We all have lots to learn from each other, and finding answers to our many challenges is going to have to be a joint venture.
Finally, this article has been written for anybody involved in racing to understand, but covering material such as this for a broad audience is challenging. So, if there are still pieces that you find obscure, reach out for help in interpretation. The answers may be closer than you think!
Oyster
And what about Oyster? Her career was short. Perhaps, had we known precisely what was going on, we might have been able to treat her, or at least withdraw her from racing and avoid a death during work with all the associated dangers—especially to the rider and the associated welfare concerns.
Had we had the tools, we might have been able to confirm that whatever the underlying cause, she had cardiac problems and was perhaps predisposed to an early death during work. With all the other studies going on, and knowing the issue was cardiac, we might have been able to target her assessment to identify specific issues known to predispose.
In the future, greater insight and understanding might allow us to breed away from these issues and to better understand how we might accommodate individual variation among horses in our approaches to selection, preparation and competition. There might be a lot of Oysters out there!
For further information about the work being undertaken by the University of Guelph
Contact - Peter W. Physick-Sheard, BVSc, FRCVS.
Professor Emeritus, Ontario Veterinary College, University of Guelph - pphysick@uoguelph.ca
Research collaborators - Dr Glen Pyle, Professor, Department of Biomedical Sciences, University of Guelph - gpyle@uoguelph.ca
Dr Amanda Avison, PhD Candidate, Department of Biomedical Sciences, University of Guelph. ajowett@uoguelph.ca
References
Caswell, J.I. and Williams K.J. (2015), Respiratory System, In ed. Maxie, M. Grant, 3 vols., 6th edn., Jubb, Kennedy and Palmer’s Pathology of Domestic Animals, 2; London: Elsevier Health Sciences, 490-91.
Hinchcliff, KW, et al. (2015), Exercise induced pulmonary hemorrhage in horses: American College of Veterinary Internal Medicine consensus statement, J Vet Intern Med, 29 (3), 743-58.
Rocchigiani, G, et al. (2022), Pulmonary bleeding in racehorses: A gross, histologic, and ultrastructural comparison of exercise-induced pulmonary hemorrhage and exercise-associated fatal pulmonary hemorrhage, Vet Pathol, 16:3009858221117859. doi: 10.1177/03009858221117859. Online ahead of print.
Manohar, M. and T. E. Goetz (1999), Pulmonary vascular resistance of horses decreases with moderate exercise and remains unchanged as workload is increased to maximal exercise, Equine Vet. J., (Suppl.30), 117-21.
Vitalie, Faoro (2019), Pulmonary Vascular Reserve and Aerobic Exercise Capacity, in Interventional Pulmonology and Pulmonary Hypertension, Kevin, Forton (ed.), (Rijeka: IntechOpen), Ch. 5, 59-69.
Manohar, M. and T. E. Goetz (1999), Pulmonary vascular resistance of horses decreases with moderate exercise and remains unchanged as workload is increased to maximal exercise, Equine Vet. J., (Suppl.30), 117-21.

Cardiac rhythm
When a horse runs badly, lameness or respiratory disease tends to immediately spring to mind, and indeed these are the most common causes—in that order. The heart comes in third, albeit quite a way behind these other body systems. If sudden death occurs in an equine athlete, a heart problem is usually the first thing that’s suspected. A new study, published in The Equine Veterinary Journal, provides significant insights on the cardiac rhythm abnormalities that can develop during and after racing in Standardbreds.
CLICK IMAGE TO READ FULL ARTICLE